

Burnout: Why It's Time to Take It Seriously
- EK Wills

- Apr 20
- 4 min read
A Preview of Groundbreaking Work Being Presented at a National Psychiatry Congress This May

When I returned to university as a mature-age student to study medicine, I had three children under ten and a daily commute from Sydney to Wollongong. On clinical placement, a supervisor told me he wouldn't have selected me — insufficient return on investment, he said, given my age, gender, and role as a mother.
By the end of the placement, he conceded I had done three times the work of the other students.
I share that story because it captures something most of us already know: the people most likely to be burnt out are often the least expected to need help — and the least supported when they do.
This May, I will be presenting at Australia's national psychiatry congress on a topic that affects far more people than it ever makes the news: burnout — not just in doctors, but in parents, carers, and women navigating midlife — and what we can actually do about it.
Australia Has a Burnout Problem
You’ve probably heard me talking about burnout for a while now.
Australian workers have been reported to have among the highest rates of burnout in the world. Yet burnout is rarely treated with the clinical rigour it deserves. Much of the support on offer comes from wellness influencers who, with the best of intentions, lack the clinical expertise to recognise when someone needs more than a journalling practice.
When burnout goes unaddressed, it doesn't plateau. People who score highly on burnout scales without structured help tend to stay there — developing chronic exhaustion, impaired function, and in some cases, depression, anxiety, and suicidal thinking. This is the gap that needs to close.
So What Actually Is Burnout?
I get asked this a lot — and it's a fair question, because for years the answer has been frustratingly vague.
The World Health Organisation defines it as profound exhaustion, a growing sense of distance or cynicism toward your work, and reduced performance. The ICD-11 calls it an occupational syndrome — something caused and kept alive by chronic, unrelenting role-related stress. Not a character flaw. Not laziness. A syndrome with a mechanism.
Here's where it gets complicated for clinicians: burnout doesn't sit in the DSM-5 as a standalone diagnosis. That single fact has quietly blocked people from accessing funded care for years. But it doesn't have to. Burnout maps closely onto Adjustment Disorder — emotional and behavioural symptoms in response to an identifiable stressor, with impaired function and distress that outweighs what you'd expect. That framing opens the door to funded inpatient care through private health insurance. For someone who has spent years being told their burnout is "just stress," that is not a small thing.
What Treatment Could Actually Look Like
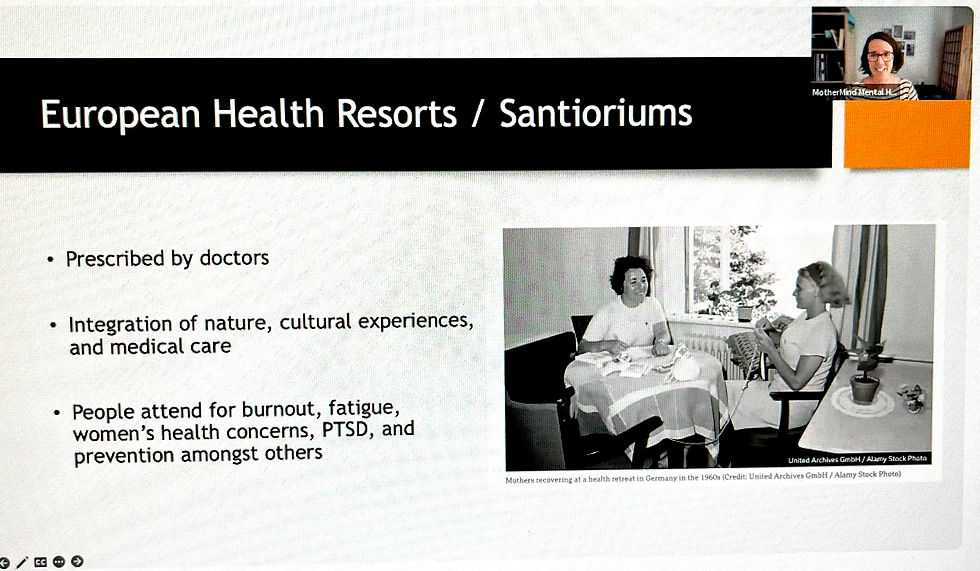
The Germans, as it turns out, figured this out decades ago.
Germany's tradition of Kur — medically prescribed, health-insurance-funded curative retreats — has existed since the 1960s. Parents and carers access immersive residential programmes in dedicated health towns: proper rest, structured therapy, nature, time. Most participants report lasting, meaningful change. It is not a luxury. It is prescribed.
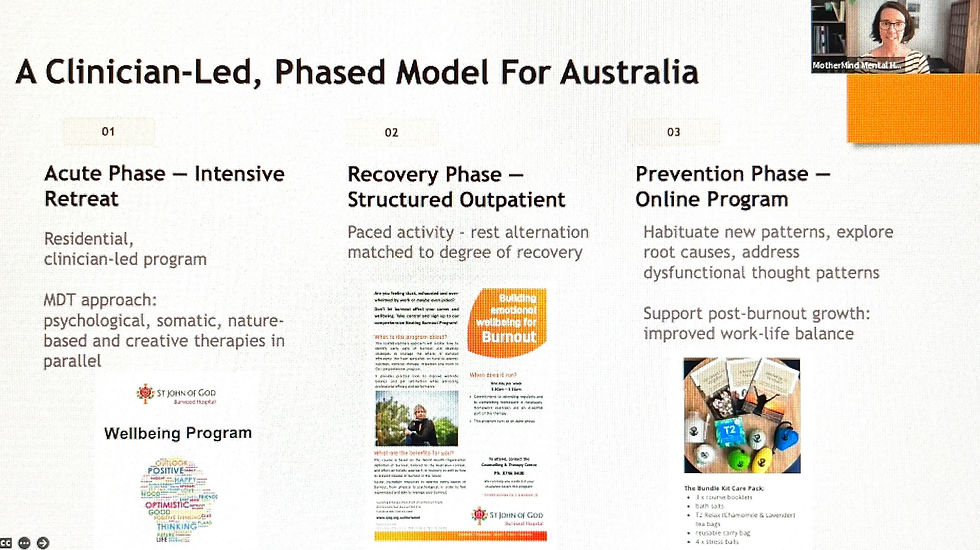
That is the inspiration behind a clinician-led, three-phase model I have been
developing and piloting here in Australia:
1. An intensive inpatient retreat — a circuit-breaker, removing the person from their stressor for focused recovery and skill introduction
2. A structured outpatient recovery phase — a paced, multidisciplinary team programme to build on those foundations
3. A take-home digital pack — to maintain gains and reinforce new patterns over time
The goal is not just feeling a bit better. It is sustainable recovery — prescribed by doctors, overseen by psychiatrists, covered by private health insurance or workers' compensation, and designed to work in the real world.
The People Who Need This Most: Parents and Carers
Close to 10% of parents and carers experience parental burnout — emotional exhaustion, feeling like a shadow of the parent you used to be, and withdrawing from the people you love most. For parents of children with mental health challenges, the risk is higher still.
One reason parental burnout resists conventional treatment: the barriers to seeking help are symptoms of the condition itself — inability to make decisions, lack of initiative, and the ingrained drive to put the caring role before everything else. Telling someone burnt out to "book an appointment" misunderstands the problem entirely.
There is also an intergenerational cost. When a parent is burnt out, their capacity to emotionally engage with their child is diminished — affecting attachment and the child's long-term mental health. Burnout in a parent is a family health issue.
The model I am proposing creates a unique clinical window: when a child is in hospital, a parent's responsibilities are temporarily reduced. That is precisely the moment to offer intensive, structured care — removing barriers that a weekly outpatient appointment simply cannot.
Women in Midlife: A Group Too Often Dismissed
Burnout and perimenopause share a striking overlap in symptoms — exhaustion, brain fog, emotional depletion, sleep disruption. Women have been misdiagnosed, or dismissed entirely, for years before accessing the right care.
The data is confronting: perimenopausal women face a nearly seven-fold increased risk of suicidal ideation compared to women before or after this transition — independently of any prior mental health history.
In January 2026, the RANZCP formally submitted to the Australian Senate Inquiry into menopause and perimenopause, calling for improved recognition of mental health during this stage of life.
This is not a wellness gap. It is a patient safety issue.
What Comes Next
The evidence for this work exists. The funding pathways can exist. What is being built now is the clinical framework to make it real — and accessible — in Australia.
If you have ever found yourself utterly depleted, unable to make decisions, going through the motions, or feeling trapped in a role with no visible exit —you may be experiencing something that deserves proper clinical attention, not just a wellness retreat as a quick fix.
That is what this work is about: a pathway where burnt-out parents, carers, workers, and women in midlife can access structured, evidence-based, medically-led care — the same standard we would offer for any other chronic condition.
The conversation starts in May. Hopefully, the change follows.
Dr Kate Wills is a psychiatrist and advocate for evidence-based approaches to burnout. She will be presenting this work at the RANZCP Congress in May 2026.


Comments